It is so established by Mother Nature that each organ performs its assigned function in the body. Gradually, with the development of science, humanity has studied every organ and its importance in our body. Only with the advent of ultrasound equipment did doctors have the opportunity to look into the secret world of the origin of life, but this only added new questions that needed answers. One of these mysteries was the then unknown organ, the yolk sac.
By order of the Ministry of Health of the Russian Federation, all pregnant women registered at antenatal clinics at their place of residence are required to undergo ultrasound screening three times for different terms gestation:
- 10-14 weeks;
- 20-24 weeks;
- 30-34 weeks.
The first ultrasound examination is carried out from 10 to 14 weeks. But for more accurate data, it is better to do an ultrasound at the end of the first trimester. During this period, it is easier to detect abnormalities in the development of the embryo, and in the case of serious defects, it is safer for the woman’s health to get rid of the abnormally developing fetus.
An ultrasound scan, which is performed before the first screening, is carried out only to establish pregnancy. And we are unable to detect any pathologies or abnormalities, because in a short period of time the size of the fertilized egg cannot allow this.
But the doctor can prescribe ultrasound examination if necessary more than three once.
Examination with a device using ultrasonic waves is carried out in two ways: through the abdominal wall or through the vagina.

Ultrasound in the first trimester is assessed according to the following indicators:
- Coccyx-parietal size. This is the size of the embryo from the crown to the tailbone. Every doctor has a table of the relationship between embryonic length and gestational age. KTE depends entirely on the period.
- Heart rate. This criterion allows us to identify congenital pathologies of the cardiovascular system. The doctor also has a table of normative indications that can be used to determine early hypoxia and heart defects.
- Thickness of the collar space. This is the length of the area between the skin of the embryo and soft tissues cervical vertebrae. The indicator helps to identify terrible diseases such as. The nuchal translucency disappears after 14 weeks of conception.
- Position of the chorion. Doctors call the placenta in the first trimester chorion. This standard indicates in which part of the uterus the fetus has taken its place.
- Nose bone size. Like other criteria, the length of the nasal bone during screening will help identify abnormalities in the development of the baby. If ossification of the bridge of the nose is not detected or it is too small, then this indicates a chromosomal abnormality. If no other violations are found, then there is no reason to panic.
- Yolk sac. This indicator is of particular importance as it helps to detect an undeveloped pregnancy. There is a certain thread between the yolk sac and the result of gestation.
In addition to studies using ultrasound equipment, in the period from 10 to 12 weeks they do. Blood sampling must be taken on the same day on which the ultrasound was performed. The analysis will reveal the likelihood of having a child with chromosomal abnormalities.
What is a yolk sac?

The yolk sac or gestational sac is a circular sac attached to the abdominal cavity of the embryo. Inside the sac is the vital yolk, which plays a vital role in the development of the fertilized egg during placentation.
This organ is present in many mammals, birds, fish and cephalopods in the early stages of development and remains throughout life in the form of a cyst-shaped process in the intestine with remaining yolk.
Main functions of the yolk sac
Without this small bubble, the full development of the fertilized egg is impossible. It takes on many functions, including nutrition and respiration of the embryo, while the appropriate organs for this are absent.
In addition to nutrition and respiration, the membrane membrane with the yolk serves as the primary circulatory system, through which oxygen and nutrients are transferred to the embryo.
Yolk sac during pregnancy

The gestational sac is evidence of a healthy intrauterine pregnancy. During ectopic gestation, this membranous membrane is not visualized. The “bag” appears in the second week of embryonic development and protects the fetus almost until the end of the first trimester, until other organs begin their work.
Between the fifth and sixth weeks, the sac should be clearly visible on ultrasound. This is one of the important criteria proper development embryo. The average diameter of the membrane shell is 5 mm.
Between the seventh and tenth weeks, the size of the bubble normally reaches up to 6 mm in diameter.
After 10 weeks, the yolk sac gradually ends its activity and must necessarily decrease in size. By the beginning of the second trimester, the fully formed placenta takes over the function of nutrition and breathing, and the yolk membrane is absorbed into the fetal cavity and in its place only a small appendage remains in the umbilical cord area.
Yolk sac norms by week

The gestational sac appears in the second week after conception; it is visible on the ultrasound monitor only in the fifth and sixth weeks. During the research, doctors determined the norms for the diameter of the yolk sac based on the timing of embryo development. These norms are considered signs of a favorable pregnancy:
- In the fifth week – 3 mm.
- At the sixth week – 3 mm.
- In the seventh week – 4 mm.
- At the eighth week - 4.5 mm.
- At the ninth week – 5 mm.
- At the tenth week - 5.1 mm.
- At the eleventh week - 5.5 mm.
- At the twelfth week - 6 mm.
- At the thirteenth week - 5.8 mm.
After 10-12 weeks, the gestational sac begins to decrease in size.
What does not visualizing the yolk sac indicate?
Modern equipment makes it possible to detect and reduce the risk of complications during pregnancy at any stage. If, during the examination, the yolk “vesicle” is not visualized during the period between six and ten weeks, this indicates an unfavorable course of pregnancy. Because this organ can accurately assess the state of development of the embryo.
The absence of a gestational sac is a sign of a missed or undeveloped pregnancy. In case of a frozen pregnancy, urgent cleaning of the uterine cavity is necessary, but it is necessary to first conduct repeated studies after 7 days to ensure the accuracy of the diagnosis.
An undeveloped gestational sac in the fertilized egg often indicates a lack of the hormone progesterone. Timely treatment with drugs containing progesterone allows you to save the fetus and avoid subsequent complications.
What do increases and decreases mean?
Small deviations from the norm in the size of the yolk sac are not an indicator of any pathology or threat to the fetus.

A belated decrease towards the end of the first trimester indicates the slow resorption of an already unnecessary organ. Additional examination is necessary after 7 days to ensure that there are no abnormalities in fetal development. If there are no pathologies and all other indicators are normal, then there is no reason to worry either. If any abnormalities are detected, cleaning the uterine cavity is recommended. The shorter the period, the safer it is for the mother’s health.
An increase in the size of the yolk sac above normal also does not immediately indicate an existing pathology. Diagnostics are required to determine possible causes. Taking certain medications, poor diet and stress can cause an increase in the diameter of the yolk sac. Or simply an individual feature that does not portend any threat to the fetus. The doctor must perform a repeat ultrasound to clarify and confirm the diagnosis.
An increase, decrease, irregular shape or compaction of the shell with nutritious yolk from the established standards is significant only in conjunction with violations of other indicators.
Is your yolk sac the right size for your due date?
YesNo
When conducting the very first ultrasound examination, which is done when menstruation is delayed and in order to accurately diagnose the presence of intrauterine pregnancy, the fertilized egg can be examined. It is when the doctor sees this miniature formation on the monitor that he already informs the woman that she will soon become a mother. On the monitor you can see the fertilized egg, which is a small oval-shaped formation. In the early stages, the embryo, which will subsequently develop and grow in the fertilized egg, is not yet visualized, but soon it will grow up, and then it will be possible to clearly see it.
An empty fertilized sac is an egg without an embryo when pregnancy does not develop. The embryo is often visible from the fifth week of pregnancy, but sometimes there are cases when this period doctor at ultrasound examination does not see the embryo, in such a situation a repeat ultrasound is prescribed. Very often, a repeat ultrasound shows both the embryo and its heartbeat. When the embryo is not visible after six to seven weeks, then, unfortunately, there is a high risk that the pregnancy will not develop. In this article we will look at the norms of the fertilized egg by week.
What is a fertilized egg
fertilized egg- these are the embryonic membranes and the embryo. This period of pregnancy is its first stage of development. And it all starts with the fusion of two cells – male and female.
 Then the fertilized egg actively begins to divide, first into two parts, then into four, and so on. The number of cells, like the size of the fetus, is constantly growing. And the entire group of cells that continue the division process moves along the fallopian tube to the zone of its implantation. This group of cells is the fertilized egg.
Then the fertilized egg actively begins to divide, first into two parts, then into four, and so on. The number of cells, like the size of the fetus, is constantly growing. And the entire group of cells that continue the division process moves along the fallopian tube to the zone of its implantation. This group of cells is the fertilized egg.
Having reached its goal, the fertilized egg attaches to one of the walls of the woman’s uterus. This occurs a week after fertilization. Until this time, the fertilized egg receives nutrients from the egg itself.
- Fertilized egg 2 weeks after insertion into the uterine cavity, it nourishes the swollen mucous membrane of this reproductive organ, which is already prepared for the process of development and nutrition of the fetus until the time of formation of the placenta.
- The baby's place, or placenta, is created from the outer shell ovum at 3 weeks, which at this time is already densely covered with villi. These villi at the site of attachment of the fertilized egg destroy a small area of the uterine mucosa, as well as the vascular walls. Then they fill it with blood and immerse it in the prepared area.
- In general, the fertilized egg is the very first sign of a normally ongoing pregnancy. It can be examined by ultrasound after two weeks of missed menstruation. Usually in this case it is visible fertilized egg 3-4 weeks. The embryo becomes noticeable only at 5 weeks of pregnancy. However, if the doctor diagnoses the absence of an embryo in fertilized egg 5 weeks- in other words, an empty fertilized egg, then the ultrasound is repeated again after a couple of weeks.
- Usually in this situation, at 6-7 weeks, the fetus and its heartbeat begin to be visualized. When fertilized egg at 7 weeks is still empty, this indicates a non-developing pregnancy. In addition to this complication, others may appear in the early stages of pregnancy - incorrect location of the fertilized egg, its irregular shape, detachments, and others.
- It is for this reason that it is important to undergo an ultrasound examination as early as possible, so that the situation can be changed if it can be corrected. Since in the first trimester ( fertilized egg up to 10 weeks) there is a high probability of spontaneous miscarriage, detachment and other pathologies. However, enough about the sad things.
Fertilized egg at 6 weeks and before this stage of pregnancy has oval shape. And an ultrasound examination usually evaluates its internal diameter - the SVD of the fetal egg. Because ovum size 7 weeks or at another stage of pregnancy is a variable value, that is, the error in identifying the gestational age using this fetometric indicator.
On average, this error is 10 days. Gestational age is usually determined not only by this indicator, but also by the values of the coccygeal-parietal size of the fetus and other indicators, which are also very important
Diameter of fertilized egg by week
When the fertilized egg has a diameter of 4 millimeters, this indicates a fairly short period of time - up to six weeks.
- Often they are fertilized egg size 4 weeks. Already at five weeks, the SVD reaches 6 millimeters, and at five weeks and three days the fertilized egg has a diameter of 7 millimeters.
- At the sixth week, the gestational sac usually grows to eleven to eighteen millimeters, and the average internal size of the gestational sac of sixteen millimeters corresponds to a period of six weeks and five days. At the seventh week of pregnancy, the diameter ranges from nineteen to twenty-six millimeters.
- Fertilized egg at 8 weeks increases to twenty-seven to thirty-four millimeters. At this stage, the fetus can be clearly seen on ultrasound.
- Fertilized egg 9 weeks grows to thirty-five to forty-three millimeters.
- And at the end of the tenth week, the fertilized egg measures about fifty millimeters in diameter.
As you can see, fertilized egg at 4 weeks It differs very much in size during the tenth week.
The question of how quickly the fertilized egg grows can be answered with confidence: until the fifteenth to sixteenth week, its size increases by one millimeter every day. Further, the diameter of the fertilized egg increases by two to three millimeters per day.
Average size of the fertilized egg in the first trimester of pregnancy
| Date of last menstruation (weeks) | Time at conception (weeks) | Inner diameter (mm) | Area (mm 2) | Volume (mm 3) |
| 5 | 3 | 18 | 245 | 2187 |
| 6 | 4 | 22 | 363 | 3993 |
| 7 | 5 | 24 | 432 | 6912 |
| 8 | 6 | 30 | 675 | 13490 |
| 9 | 7 | 33 | 972 | 16380 |
| 10 | 8 | 39 | 1210 | 31870 |
| 11 | 9 | 47 | 1728 | 55290 |
| 12 | 10 | 56 | 2350 | 87808 |
| 13 | 11 | 65 | 3072 | 131070 |
In early pregnancy, an ultrasound is performed to identify a viable embryo in the uterine cavity, confirm the gestational age, exclude pathology of the embryo, or identify normal variants, such as multiple pregnancies.
The initial sign of pregnancy is thickening of the endometrium, but ultrasound does not tell what exactly causes this thickening.
When using a high-resolution transvaginal sensor, a fertilized egg with a diameter of 1 mm is visualized in the uterine cavity 4 weeks and 2 days after the last menstruation with regular menstrual cycle.
If menstruation is delayed for 5-7 days or more (gestational age is 5 weeks), a fertilized egg with a diameter of 6 mm should be clearly visible in the uterine cavity. It has a clear round shape with a fuzzy light rim along the periphery (hyperechoic rim - chorion). In this case, the level of beta-hCG in the blood is 1000-1500 IU/l (see What is hCG?). When the hCG level is more than 1500 IU/l, the fertilized egg in the uterine cavity should be clearly visualized.
With a lower level of hCG, the fertilized egg in the uterine cavity may not be detected by transvaginal echography. With a transabdominal examination, detection of the fertilized egg in the uterine cavity is possible at a beta-hCG level of 3000-5000 IU/l.

Fig.1Uterine pregnancy 4-5 weeks. Transabdominal scanning.
IMPORTANT: The gestational age cannot be accurately determined by the size of the fertilized egg. Many tables on the Internet with the size of the fertilized egg determine the period very approximately (see table below).
From about 5.5 weeks, transvaginal ultrasound begins to visualize an extraembryonic structure in the fetal egg - the yolk sac (eng. yolk sac). At the same time, the beta-hCG level averages approximately 7200 IU/l (see hCG norms during pregnancy).
Since the yolk sac is part of the germinal structures, its detection makes it possible to distinguish a fertilized egg from a simple accumulation of fluid in the uterine cavity between the endometrial layers, and in most cases, makes it possible to exclude ectopic pregnancy. The incidence of ectopic pregnancy is 1-2 per 2000-3000 pregnancies. Its risk increases with the use of assisted reproductive technologies (ART). An ectopic pregnancy should be suspected when hCG level is more than 1500 IU/l, and the fertilized egg is not detected in the uterine cavity.

Fig.2Pregnancy 5.5 weeks. The yolk sac is identified. Transvaginal scan.
From 6 weeks of pregnancy (sometimes a little earlier), an embryo about 3 mm long can be identified in the fertilized egg. From the same date, the majority ultrasonic devices allows you to determine the heartbeat of the embryo. If the heartbeat is not detected or is unclear when the embryo length (CTE) is 5 mm, a repeat ultrasound scan is indicated after a week. The absence of cardiac activity at this stage is not necessarily a sign of fetal distress or a non-developing pregnancy.
The numerical values of the heart rate in an embryo during an uncomplicated pregnancy gradually increase from 110-130 beats/min at 6-8 weeks of pregnancy to 180 beats/min at 9-10 weeks.
The length of the embryo is measured from the head to the tail end, and is designated under the term CTP (coccygeal-parietal size), in English. literature - CRL (Crown-Rump Length). It should be noted that the coccygeal-parietal size of the embryo is less subject to individual fluctuations than the average internal diameter of the ovum, and therefore, its use to determine the gestational age gives top scores. The error usually does not exceed ±3 days. With clear visualization of the embryo, the gestational age is determined depending on its length, and not on the size of the average internal diameter of the ovum (SVD).

To correctly measure the coccygeal-parietal size of the embryo, its clear visualization is necessary. In this case, one should strive to measure the maximum length of the embryo from its head end to the tailbone.
During normal pregnancy, the diameter of the ovum increases by 1 mm per day. Lower growth rates are a poor prognostic sign. With a gestation period of 6-7 weeks, the diameter of the ovum should be about 30 mm.
Table 1. Dependence of gestational age on the average internal diameter of the ovum (Dv), M. N. Skvortsova, M. V. Medvedev.
Table 2. Normal values of the coccygeal-parietal size (CPR) depending on the gestational age (full weeks + days), data in millimeters, the lower limit is the 5th percentile, the upper limit is the 95th percentile.

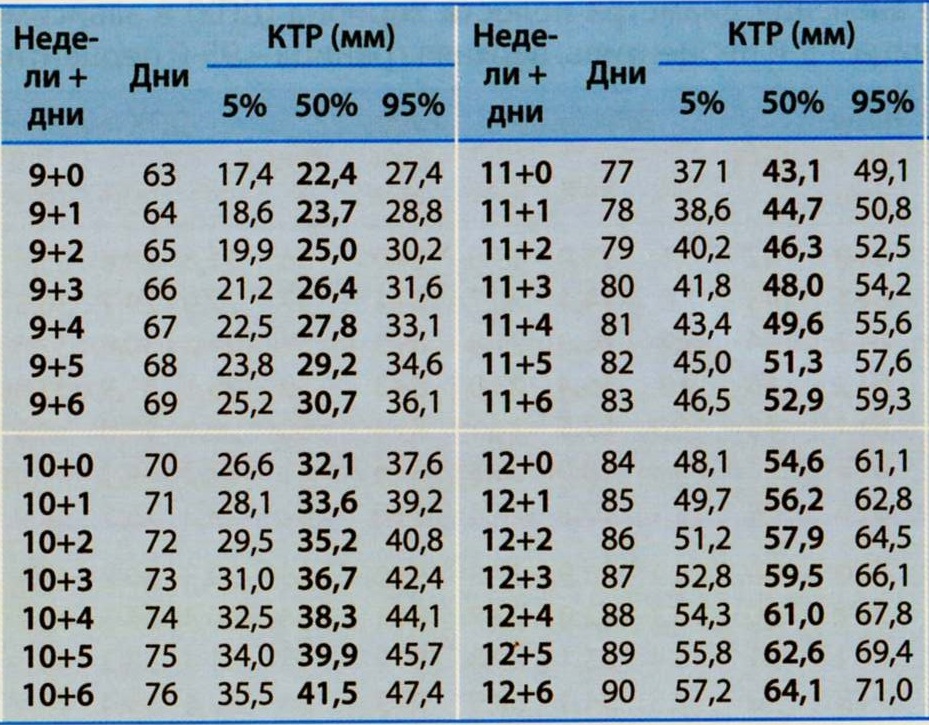
It should be emphasized that determining the gestational age by the length of the CTE is best done before 12 weeks of pregnancy. In more late dates measurements of biparietal diameter, head circumference, and abdominal circumference should be used.

Fig.3 Pregnancy 12 weeks 3 days.
The motor activity of the embryo is determined after 7 weeks of pregnancy. At first, these movements are very weak and isolated, barely noticeable during examination. Then, when differentiation into the head and pelvic ends of the embryo becomes possible, movements resemble flexion and extension of the body, then separate movements of the limbs appear. Since episodes of motor activity of the embryo are very short and count in seconds, and periods of motor rest can be significant in time, registration of the cardiac activity of the embryo is undoubtedly a more important criterion for assessing its vital activity.
The diagnosis of anembryonia (empty fertilized egg) is assumed if a yolk sac is not detected in a fertilized egg measuring 20 mm. Or if the fertilized egg with a diameter of more than 25 mm with a yolk sac does not contain an embryo. And also when the yolk sac size is 10 mm or more. In any case, if anembryonia is suspected, all data obtained should be interpreted in favor of pregnancy, and the study should be repeated after 7 days.
The diagnosis of a non-developing pregnancy should not be made if, on ultrasound, the ovum is less than 20 mm in size. When the embryo is 5 mm or more in length, in most cases the heartbeat should be clearly detectable. If the embryo is less than 5 mm, the ultrasound should be repeated after a week. If, upon repeated examination a week later, at CTE = 5-6 mm, cardiac activity is not detected, the pregnancy is not viable. The diagnosis of a non-developing pregnancy can be confirmed by a discrepancy between the beta-hCG level and echographic data.
It should be noted that the normal rate of pregnancy termination in the population is 15-20% of all clinically diagnosed pregnancies. However, in reality, if we count all “chemically” diagnosed pregnancies, determined by the level of beta-hCG before the expected next period, the miscarriage rate can reach up to 60%.

Sincerely, ultrasound diagnostics doctor, Barto Ruslan Aleksandrovich, 2012
All rights reserved®. Quoting only with the written permission of the author of the article.
The yolk sac is an embryonic organ that contains a supply of nutrients for the embryo. The yolk sac persists throughout the first trimester and resolves on its own after 12 weeks. The shape and size of the yolk sac are one of the most important indicators of the course of pregnancy in its earliest stages.
Origin
The yolk sac is formed from a special structure - the endoblastic bladder - on the 15-16th day of embryo development (or on the 29-30th day from the last menstruation). During this period, a woman may not yet be aware of her changed status, and only a delay in menstruation indicates a possible conception of a child. The yolk sac develops together with the fertilized egg and other structures of the embryo according to a program given by nature. Any deviations from the genetically programmed rhythm can lead to termination of pregnancy.
The yolk sac is a closed ring located inside the chorionic cavity. It does not function for long - only 12-14 weeks. At the beginning of the second trimester, the yolk sac begins to decrease in size. After 14 weeks, the formation disappears without a trace, having fulfilled all its functions.
Role of the yolk sac
The yolk sac is a temporary (provisional) organ, but without it the normal course of pregnancy and embryo development is impossible. On early stages The size of the yolk sac exceeds the size of the embryo and amniotic cavity. The yolk sac actively grows from 6 to 12 weeks of gestation, after which it gradually decreases in size and completely disappears.
On days 18-19 from conception, the yolk sac becomes the focus of hematopoiesis. In its walls, areas of erythropoiesis are formed, and the first red blood cells are formed. Subsequently, a branched network of capillaries is formed here. Primary red blood cells, leaving the yolk sac, enter the circulatory system of the embryo and are carried through the bloodstream throughout the body.
From the 28th day from the moment of conception, the yolk sac begins to produce primary germ cells of the embryo. Subsequently, the germ cells migrate from the yolk sac and reach the gonads (sex glands). 4-5 weeks of pregnancy is an important stage in the development of the fetal reproductive system. Any negative impacts during this period (infections, radiation, intake medicines) can disrupt the formation of the gonads of the embryo and cause infertility.
From 2 to 6 weeks of pregnancy, the yolk sac acts as a liver for the embryo. The walls of the yolk sac synthesize important proteins and enzymes necessary for the normal development of the entire organism. In particular, AFP (alpha fetoprotein) is produced here. In the fetal circulatory system, AFP binds to PUFAs (polyunsaturated fatty acids) and transports them to all cells and tissues. AFP also suppresses the immune response to newly synthesized proteins, allowing metabolic processes to proceed at the desired rhythm.
Other functions of the yolk sac:
- regulation immune system fetus;
- synthesis of hormones;
- creating conditions for adequate metabolism;
- excretion of metabolic products.
The yolk sac performs all its functions until the basic internal organs and will not take on this work. After 12 weeks there is no need for a yolk sac. By the beginning of the second trimester, only a small cystic formation at the base of the umbilical cord remains from the yolk sac.
Yolk sac on ultrasound
During ultrasound examination with a transvaginal sensor, the yolk sac is detected from 6 to 12 weeks of pregnancy. Minor deviations (up to 2 weeks) in any direction are allowed. The absence of a yolk sac on ultrasound is an unfavorable sign indicating serious problems during pregnancy.
When performing an ultrasound, the doctor evaluates the location, shape and size of the yolk sac. The size of the yolk sac will depend on the gestational age.
Yolk sac norms by week: 
It is important to remember: the size of the yolk sac changes quickly to early stages pregnancy. Minor deviations should not frighten a pregnant woman and cannot be the basis for making serious diagnoses. If the size of the yolk sac is not normal, the doctor must carefully examine the embryo, determine the location of the fertilized egg and other parameters. If necessary, a repeat ultrasound is performed after 1-2 weeks.
Time frame for ultrasound:
- 6-7 weeks;
- 12-14 weeks.
At 6-7 weeks, the first ultrasound examination during pregnancy is performed. During the procedure, the doctor confirms the fact of pregnancy and determines its duration. The doctor indicates the location of the fertilized egg (in the uterus or outside it), assesses the condition and location of the yolk sac and chorion. The size of the fetus is determined, its correspondence to the gestational age and the size of the yolk sac. At 6 weeks, the embryo's heartbeat is also listened to and its viability is assessed.
At 12-14 weeks, the first ultrasound screening is performed. During the procedure, the doctor evaluates the condition of the embryo, chorion and yolk sac. During this period, the yolk sac reaches its maximum size. When performing an ultrasound at a later date, the yolk sac begins to dissolve and is not always visualized on the screen. After 14 weeks, the yolk sac is normally not detectable.
Adverse symptoms:
- absence of the yolk sac for up to 12 weeks;
- thickening of the yolk sac more than 7 mm or decrease less than 2 mm;
- change in the shape of the yolk sac.
In combination with other symptoms, these conditions may indicate high risk termination of pregnancy in the first trimester. To clarify the diagnosis, it may be necessary additional examination on an expert-class device.
Pathology of the yolk sac
When performing an ultrasound, the doctor can detect the following conditions:
The yolk sac is not visualized
Normally, the yolk sac is detected by ultrasound in the period from 6 to 12 weeks. The absence of a yolk sac is an unfavorable sign. If such an important organ is resorbed ahead of time for some reason, the embryo ceases to receive the substances necessary for its development. The synthesis of hormones and enzymes is disrupted, and the production of red blood cells stops. With premature reduction of the yolk sac (up to 12 weeks), spontaneous miscarriage. It is not possible to maintain pregnancy with medications.
The absence of a yolk sac on ultrasound (from 6 to 12 weeks) is considered one of the signs of a regressing pregnancy. In this case, the heartbeat of the embryo is not determined, its size does not correspond to the gestational age. Treatment is only surgical. In case of regressing pregnancy, the fertilized egg is removed and the uterine cavity is curetted.
The yolk sac is smaller than normal
Possible options:
- The yolk sac is defined as a rudimentary formation.
- The size of the yolk sac does not correspond to the duration of pregnancy (smaller than normal).
Any of these situations indicates that premature resorption of the yolk sac has begun. If at the time of reduction of the sac the internal organs of the fetus are not yet formed and are not able to fully function, the death of the embryo and spontaneous miscarriage occurs. In some cases, contractions of the uterus and miscarriage do not occur after the death of the embryo. This condition is called regressive pregnancy.
The yolk sac is larger than normal
The main reason for this symptom is incorrect determination of the gestational age. This is possible with an irregular menstrual cycle (against the background of various gynecological pathologies or in nursing mothers). In this situation, the doctor should evaluate the size of the embryo and recalculate the gestational age taking into account the available data.
An important point: changes in the size, shape or density of the yolk sac are important only in combination with other ultrasound indicators. If any abnormalities are detected, the condition of the embryo (location, size, heartbeat) should be assessed. If the baby is growing and developing in accordance with the gestational age, there is no reason to worry. Changes in the yolk sac in this case are considered an individual feature that does not affect the course of the first trimester.
The embryo and the membranes surrounding it are the main initial components of the amniotic egg. As the fetus develops, the space around it also increases - this is a normal process of embryo development. Next, you are invited to familiarize yourself with key information directly about the fertilized egg, as well as regarding the features of changes in its size during pregnancy and possible pathologies formation.
As you know, fertilization occurs through the penetration of a male sperm into a female egg. After this, the active process of embryo development begins: first, the fertilized egg is divided into 2 parts, then into 4, then into 8, etc. As the number of cells increases, the embryo itself grows. Without stopping to develop, the embryo moves towards its destination, which is normally the cavity of the female uterus. It is the mentioned group of cells that represents the fertilized egg in question. 
Once the desired location is reached, the embryo is implanted into the wall of the uterus. On average, this process takes up to 7-10 days after the sperm penetrates the egg. Until reaching its destination, nutrition of the fertilized egg is provided directly by the egg, and after consolidation, by the uterine mucosa.
Over time, the functions of providing nutrition to the embryo are taken over by the placenta, which is formed from the outer layer of the fertilized egg. Directly on the mentioned outer layer there are so-called. villi, which ensure implantation of the embryo in a suitable place. 
The formation and successful consolidation of the fertilized egg is the main sign normal course female pregnancy. On average, the embryo becomes visible during ultrasound examination 5 weeks after the missed period, while the fertilized egg can usually be seen after 2 weeks. If during the first ultrasound the doctor sees the so-called. empty ovum, after a couple of weeks the test is repeated. 
Normally, the embryo is visualized by the 6-7th week of pregnancy. During the same period, his heartbeat is usually noticeable. If there is no embryo in the ovum during repeated ultrasound examination, a non-developing pregnancy is diagnosed. 
In view of this, if menstruation is delayed, a woman should have an ultrasound scan as early as possible in order to promptly detect existing abnormalities and, if such a possibility is present, undergo treatment to eliminate the identified problems.
When assessing the condition of the ovum, the specialist first of all pays attention to its shape and internal diameter. During the first weeks, the shape of the fertilized egg is close to oval. By assessing the internal diameter, the doctor can draw conclusions about the expected gestational age. Along with this, not every woman’s fertilized egg has the same size, so when determining the gestational age, an error often occurs, averaging one and a half weeks. For more accurate results, fetal CTE and other diagnostic measures are assessed. 
 Features of the growth of the fertilized egg
Features of the growth of the fertilized egg
As noted, the size of the fertilized egg, in the absence of various kinds of pathologies, is constantly increasing.

More detailed weekly information regarding the normal size of the gestational sac is given in the following table. 
Table. Sizes of fertilized egg by week
Possible developmental disorders of the ovum
Under the influence of certain factors, the development of the fertilized egg can occur with certain pathologies. You can find a description of the most commonly diagnosed anomalies in the following table.
Table. Pathologies of development of the ovum
| Pathologies | Description |
|---|---|
| Form violations | The shape of the fertilized egg in both scans up to 5-6 weeks is usually round. By 6-7 weeks, the fetal egg becomes oval in a longitudinal scan, but remains round in a transverse scan. Along with this, the development of form can occur with various kinds of deviations. Most often, this is caused by various types of tumors in the uterine cavity. Also, this pathology can occur in the case of partial placental abruption. |
| Pathologies of location | In the absence of deviations, implantation of the fertilized egg most often occurs in the fundus of the uterus or its posterior wall, sometimes in the area of the internal os or at the top of the uterus. Other options for the location of the ovum are assessed by a specialist. He also makes a decision on further actions in relation to a particular patient. |
| Dimensional violations | Information regarding changes in the size of the ovum as pregnancy progresses has been provided previously. Significant deviations from the given values in both directions are considered pathological, and conclusions about their significance are made by a specialist. |
| Functional pathologies |
It is impossible to give any definite answer regarding the causes of the development and treatment of pathologies in the development of the ovum - each case requires individual consideration by a qualified specialist. Only a doctor can objectively assess the situation and make the most appropriate decision. 
Regularly undergo the necessary examinations, follow the recommendations of your treating specialist and be healthy!
Video - Size of fertilized egg by week of pregnancy table





